75F WITH ALTERED SENSORIUM
Hello all this is G Pranay kumar rao,a eighth semester student.This E Log depicts the patient centered approach to learning
This is an online e log book to discuss our patient de-identified health data shared after taking his / her / guardians signed informed consent. Here we discuss our individual patients problems through series of inputs from available global online community of experts with an aim to solve those patients clinical problem with collective current best evident based input.
This E blog also reflects my patient centered online learning portfolio and your valuable inputs on the comment box is welcome.
History of present illness:-
Patient was apparently normal until 3pm yesterday (19/10/2023).
She then became altered since 3pm yesterday and started speaking random words, not answering revelantly and without deviation of mouth with weakness of right upper limb and right lower limb.
Associated with involuntary micturition and slurring of speech
No C/O loss of consciousness, seizures, headache, involuntary defecation, vomitings, fever, trauma, diplopia.
History of past illness:-
H/o CVA with right sided hemiparesis 3 years back, recovered now
K/C/O Hypertension since 4 years ( not using medication regularly in past few days)
N/K/C/O DM,TB, Epilepsy,CAD, Thyroid disorders, Bronchial asthma
Personal history:-
Diet - Mixed
Appetite - Normal
Bowel and bladder - regular
Sleep - adequate
No addictions
No H/o food and drug allergies
Family history:-
Not significant
General examination: -
Patient is conscious, coherent, cooperative, moderately built and nourished
No signs of pallor, icterus, cyanosis, clubbing, generalised lymphadenopathy and oedema
VITALS :-
Temp- 97.8F
BP-150/90 mmHg
PR- 68 bpm
RR - 18com
Sp02-97%
Systemic examination:
CVS- S1;52 + , no murmors
RS- BAE+ NVBS heard
P/A- Soft non tender, no organomegaly
CNS :-
Patient is arousable
No signs of meningeal irritation
Tone:
Right. Left
UL Increased. Increased
LL. Increased. Increased
Power:
Right. Left
UL. 2/5. 3/5
LL. 2/5. 3/5
Reflexes. Rt. Lt
-Biceps. 3+. 3+
Triceps. 3+. 3+
Supinator 2+. 2+
Knee. 3+. 3+
Plantar. extension extension
INVESTIGATIONS ;-

 |





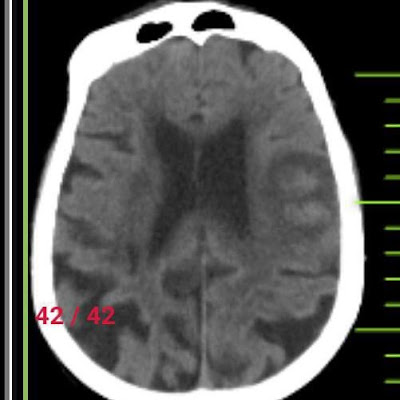
PROVISIONAL DIAGNOSIS
Recurrent CVA asso with right side Hemiparesis with Hemorrhagic infarct in Left fronto parietal region
TREATMENT
19/10/2023
1) RT feeds - 100 ml H20 2 hrly
200 ml milk 4 hrly
2) IV fluids NS @30 ml / hr
3)inj mannitol 100ml IV /TID ( 8am , 2pm, 8pm )
4)inj levipil 500mg IV/BID ( 8am ,8pm )
5) vitals monitoring houlrly
6) inform SOS
20/10/2023
1) RT feeds 100 ml water 2 hrly
200ml milk 4 hourly
2)IVF NS @50ml/hr
3)Inj Mannitol 100ml IV /TID
4)inj levipil 500mg iv/bid
5)inj pantop 40mg IV
21/10/2023
IV fluids NS, DNS @ 50ml/ hr
Inj. Mannitol 100ml i.V/TID
Inj. Levipil 500mg iv/bd
Tab.Amlong 5mg PO/CD
Syrup. Potchlor 10ml in 1 glass water po/tid
GRBS 4th hourly monitoring
Vitals monitoring hourly


